

Why am I writing this?
Alcohol, Tobacco and other Drugs have, in one way or another been a very significant part of my life. Let me start from the beginning: I started smoking a few cigarettes in early adolescence and became a more regular smoker in my late teens when I went to University. It was at this time in my life that I also began to enjoy a few beers on a regular basis This prompted me to begin, what would become an absorbing pastime, home wine and beer making. The equipment and ingredients were cheap and the resulting alcoholic beverages

were of remarkably high quality. Indeed, some of my products won awards in amateur winemakers’ competitions. I look back on this hobby as an example of timeless simplicity! In my early 20’s, my love affair with cigarettes ended, when I discovered the joys of pipe smoking. In those halcyon days there was no real market in Ireland for “street” drugs and, as a result, I and my friends never even considered using drugs.
My subsequent career as a Social Worker provided me with considerable direct evidence of the risks associated with smoking and drinking, but I felt confident that due to my moderate consumption of both substances, I could safely continue to enjoy these indulgences. Eventually, the growing evidence about the risks of smoking became so compelling that I quit. Later, when I went to work with an Drug & Alcohol Dependence service, the severity of the problems that my clients were experiencing, made such an impact on me,
that I stopped drinking altogether for two years! I then resumed moderate drinking, feeling assured that I could stop anytime I wanted to. Nevertheless, some 20 years later, I had to face the fact that my consumption of alcohol had gradually increased to a level which was clearly excessive and I was regularly suffering from bouts of depression and anxiety. Alcohol had become a burden instead of a pleasure and after seeking medical advice, I realized that I should either reduce my drinking or stop altogether. I began a medically supervised controlled drinking program but after a number of unsuccessful attempts to moderate my drinking, it became clear that I should ” bite the bullet” and become abstinent. I felt confident that, although this might not be pleasant, it would be manageable: after all, I had done it before. I started treatment with a psychiatrist who specialized in alcohol misuse problems and joined Alcoholics Anonymous. Even with this intensive treatment and support, it took quite a long period of on and off drinking before I was able to sustain my current period of protracted abstinence. Looking back over earlier years, I have to say that I really did enjoy smoking my pipe, drinking Guinness and savoring wines from around the world. For some years I mourned the loss of these indulgences. However I was eventually able to move on and discover other pleasures. There is considerable evidence that if I were to resume drinking, my previous pattern of alcohol misuse would return along with the anxiety and depressed which had dogged me. Consequently, I have a strong focus on avoiding environments, behaviors, stressors and any kind of emotional negativity that might trigger my return to drinking. Having finally been released from the burden of alcohol misuse. I am determined to do everything possible to avoid returning to that dark place.
My professional experience of working with alcohol and drug related problems, provides a different perspective to my learned experience of substance abuse. Indeed, I would go as far as saying that the use and misuse of alcohol, tobacco and other drugs has, in one way or another, been a key dimension of my life experience. This is why I am writing this opinion piece.
Why are Alcohol, Tobacco and Other Drugs (ATODS) so popular ?
There seem to be a few key reasons :
- Enjoyment
- Dealing with emotional distress
- Behaviour learned from family members and/or peer groups
- Social connection
- Cultural influences
- Encouragement by manufacturers and suppliers (both legal and illegal)
Enjoyment. Tobacco, alcohol and street drugs are all toxic psychoactive substances that trigger a series of complex neurochemical changes in the user’s brain and other parts of the central nervous system and elicit a range of pleasurable feelings. The consumption of a sufficiently high dosage will however, cause unpleasant toxic reactions which in some circumstances can be life threatening. Most of us soon learn what sort of effects we can expect when we use a particular substance and try to adjust our level of consumption, so that our enjoyment is not marred by the pain of toxicity. Learning about the effects of alcohol and drug use can sometimes have a novel and unexpected consequence. It may be possible for some people to experience the pleasurable feelings which they anticipated, even when substance they are using is actually inert: a kind of placebo effect.
Social learning. Many people first become aware of substance use by watching their family, friends and peers smoking, drinking and using drugs. Then wittingly or unwittingly they may start to imitate them. I have met many people who saw, at first hand, the problems caused by the substance abuse of those close to them and had sworn never to go down that path. Paradoxically, that’s exactly what many of them did.
Social connection. Sharing food, alcohol and tobacco have traditional ways of initiating and sustaining social connections.
Alcohol is particularly useful in this way as it can reduce inhibitions and lessen social anxiety. It’s no wonder that having wine and beer on hand is recognized as an effective method of encouraging interaction at most kinds of social gatherings.
Stress, Anxiety and Depression. Many people self-medicate by drinking alcohol, using street drugs, or abusing prescribed medication. During difficult times smokers may increase the tempo of their habit and recovered smokers may relapse. Substance use does provide a degree of, short term, relief from distress associated with illness or other troubling personal circumstances.
Cultural Influences In most societies the use of tobacco, alcohol and other drugs is regulated by a combination of social pressures and legal regulation. Some societies take a somewhat laissez-faire approach and intervene only when absolutely necessary. In others the use of intoxicating substances is subject to strict social and legal constraints (e.g. Islamic prohibition of Alcohol) .

Since supplies of rum and wine were unloaded from the ships of the First Fleet the use of alcohol has been a visible and celebrated part to Australian society. Enjoying a few drinks (or in some cases quite a few drinks) has been part of the Australian male identity. This was apparent when I and my family moved to Australia in the 1970’s.
The term “wowser” (a puritanical or censorious person) was sometimes used to describe a man who abstained from alcohol. Traditionally, Australian women have been more moderate drinkers and have had a greater number of teetotalers amongst their ranks. During recent decades Australian attitudes to alcohol consumption seem to have moderated.
For many years, Smoking was widespread in Australia, particularly amongst males. Indeed, a tea break in Australia has traditionally been referred to as “smoko”. When I arrived in Australia, I noticed lots of people smoking in shops, offices and other public facilities . A senior colleague in my first Australian workplace was a “chain smoker” who would smoke continuously during most staff meetings. On one occasion I decided to make a statement by eating an orange during the meeting, but was taken to task for being ill-mannered. I retorted that “at least it’s not unhealthy”. My senior colleague laughed and continued smoking. In recent years, however, smoking seems to have become much less socially acceptable in Australia. This cultural change may have been due, at least in part, by the introduction of far reaching public health restrictions.
The use of street drugs in Australia is illegal and has generally been regarded as seriously deviant behavior, although attitudes are softening regarding the use of marihuana. Younger Australians are probably more accepting of the use of street drugs than their elders. Its possible, also to identify specific Australian sub- cultures, where the use of street drugs is woven into the fabric of day to day life. These groups tend to have their own drug related, lexicon, values and behaviors.
Encouragement by Manufacturers and Suppliers. There’s lots of of money to be made from the production, distribution and sale of tobacco, alcohol and street drugs. Alcohol and tobacco manufacturers have promoted their products through massive advertising on billboards and in the printed and broadcast media.
They have used sports sponsorship and other promotional strategies to increase their market share. In recent years Australian governments have introduced far reaching public health measures to limit the advertising and promotion of tobacco products and smoking in public places is now prohibited. This public health measures seem to have been effective in decreasing the rate of smoking.
The “street drug” industry manufactures products that are in high demand. and is also involved in the sale of improperly obtained prescription drugs. Free from government regulations and taxation, this is an exceptionally lucrative business. Cashed up investors stand to make a fortune and whilst there is some possibility that the authorities may become aware of their activities, it is their retail operatives who are at much higher risk of arrest and imprisonment. It’s probably not difficult to recruit people for the street drug sales force: no qualifications, work experience or character credentials are necessary and un-regulated sales and credit control techniques can be employed to ensure that the customers needs are met and that the goods are paid for. For some people it can really seem like the only, readily available, way to make some money.
Alcohol, Tobacco and Drug usage in Australia “now and then”.
Tobacco use in Australia had begun some years before European settlement. It had been introduced to the indigenous population in Arnhemland by visiting Indonesian fishermen. Soon after the arrival of the First Fleet, Australian tobacco cultivation began and people lit up . It is likely that part of early crops was used to make pesticide to counter insect infestation of sheep. Commercial cultivation reached its peak in the early 1970s, and after gradual decline tobacco Australian farming finally terminated in 2006.
The most recently available data suggests that around 14% of Australians over 14 yrs currently smoke, 22.8% are ex-smokers and 63.2 have never smoked. 4% of young people aged 12-15 are smokers, and for those aged 16-17 the rate is 14%: an all time low. However, the continued decline of smoking in these younger age groups is threatened by the proliferation and uptake of novel products such as smaller factory-made cigarette pack sizes, smaller roll-your-own tobacco pouch sizes, and e-cigarettes.
The risks associated with tobacco use are now well recognized. Research estimates that two in three lifetime smokers will die from a disease caused by their use of tobacco. The most recent estimate of annual deaths caused by tobacco in Australia is a staggering 20,933 . This includes deaths from active smoking and from exposure to secondhand smoke.
On face value daily “social smoking” may see a lot less hazardous than regular smoking. However there is emerging evidence that casual tobacco use may pose some of the same cardio-vascular risks as daily smoking.
As someone who smoked regularly of 18 years, I can confirm how difficult it is to escape from the clutches of tobacco dependence. Initially I experience many of the characteristic physical withdrawal symptoms as my body struggled to adjust to the absence of nicotine:
- Feeling irritated or upset
- Feeling jumpy or restless
- Difficulty in concentrating
- Difficulty in sleeping
- Hunger/weight gain
- Feeling anxious, sad or depressed
I also struggled with a variety of behavioral and psychological withdrawal symptoms. I missed the ritual of preparing my pipe for smoking, the comfort of feeling it clamped between my teeth and belonging to a tradition of contemplative pipe smoking.
The total burden of ill health associated with tobacco use, surpasses that of any other toxic recreational substance. There is no safe way to use tobacco products.
Over the years I have met quite a few smokers who have developed serious tobacco related illnesses including heart disease, strokes, limb amputations and various cancers. Some have become progressively incapacitated whilst others have died prematurely. My message to smokers is simple: quit! To those who are flirting with tobacco -walk away now before you become hooked! The total burden of ill health associated with tobacco use, surpasses that of any other toxic recreational substance. There is no safe way to use tobacco products.
Alcoholic drinks contain various concentrations of ethyl alcohol (also called ethanol, grain alcohol, drinking alcohol, or simply alcohol). Ethyl alcohol is a naturally occurring substance which is obtained when the sugars and starches found in fruit, vegetables and grains are fermented using yeast. The basic beer production process involves the fermentation of barley using yeast with the addition of hops for flavoring. From medieval times until the 19th century low alcohol beer called Small Beer, a type of weak beer was the staple drink of most of the population of England in preference to water which was often dangerously polluted . Fruit (usually grapes) is fermented in the production of wine, often using the natural yeast that collects on the fruit skins.
Alcoholic spirits such as whisky, brandy, gin and vodka are made by distilling these original products of fermentation to produce relatively pure ethyl alcohol which is usually slightly diluted before being bottled for sale to consumers. Fortified wines such as port and sherry have a higher alcohol content than regular wines due to the addition of some distilled spirit.
Alcohol has had a prominent and at times notorious role in Australia’s European settlement. Barrels of wine and spirits arrived with the First Fleet and soon local manufacturing of beer, wine and spirits was established. It would not be long before Australia became known as a hard drinking nation.
“They are not a nation of snobs like the English or of extravagant boasters like the Americans or of reckless profligates like the French, they are simply a nation of drunkards.”
Marcus Clarke 1869
At the time, Clarke’s observation was understandable. During Australia’s penal era, rum had been used as currency and it was believed that the colony’s inhabitants drank more alcohol per capita that any other time in human history.
One of Australia’s most personable and popular Prime Ministers, the late Bob Hawke, had a reputation for heavy drinking and whilst completing Rhodes Scholarship studies at Oxford, he became famous for sculling a yard of ale – two-and-a-half pints, or 1.4 liters – in 11 seconds, then a world record.
Whilst this would probably have been a damaging embarrassment for public figures elsewhere, it only served to endear Hawke to many in the Australian public. It should be noted that Hawke was able abstain from alcohol during his years as Prime Minister, but returned to drinking as soon after leaving office.
Australia seems to have retained at least some of this reputation as an intemperate nation, but this view is becoming increasingly outdated. the following table compares Australians’ per capita consumption of alcohol with that of a number of comparable countries.
| Country | Liters of Pure Alcohol consumed annually by citizens over 15 yrs |
|---|---|
| Lithuania | 15 |
| Germany | 13.4 |
| Ireland | 13 |
| United Kingdom | 11.4 |
| Australia | 10.6 |
| United States | 9.8 |
| China | 7.2 |
| Israel | 3.8 |
This would suggest that, in fact, Australians consumption of alcohol is somewhat lower than that of several comparable first world countries. Perhaps, nowadays, we should instead be regarded as alcohol connoisseurs; rather than hard drinkers.
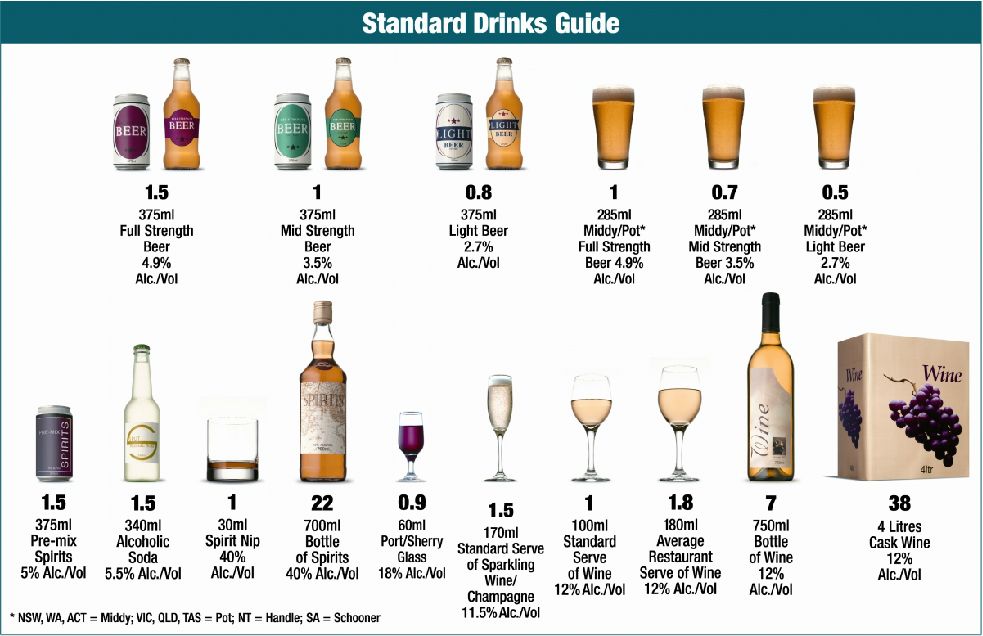
However, to get a more detailed picture of Australian alcohol consumption, it is necessary to examine how drinking patterns vary throughout the population. Individual alcohol consumption is normally measured in standard drinks. One Standard Drink equals 10 grams of pure alcohol. The following figure details the number of standard drinks contained in common Australian drinks.
The next table provides information about Australian’s average daily consumption of alcohol.
| Average number of standard drinks per day. | % of Australians over 14 years |
| None | 23.8 |
| 1-2 | 59.5 |
| 3 or more | 16.7 |
The data in these two tables reveals that the vast majority of Australians over 14 yrs (83%) either abstain or, on average, consume no more than two standard drinks per day, which almost coincides with the Australian Alcohol Guidelines’, recommendation that….. to reduce the risk of harm from alcohol-related disease or injury, healthy men and women should drink no more than 10 standard drinks a week. As the average daily consumption of alcohol increases, so do the risks of long-term harm to the cardiovascular system, gastrointestinal system and the brain and central nervous system. In fact there are few parts of the body that are immune to the toxic effects of alcohol. Of course, there is a range of factors which may potentiate harms caused by alcohol: lifestyle factors such as smoking, poor diet, lack of exercise, workplace health and safety risks, genetics, mental health and emotional problems and many more.
Increasing recognition is being given to the extent to which some specific population groups are at higher risk of alcohol related harms.
- Brain development in continues until people reach 25 years of age: perhaps longer for males. The developing brain can be adversely affected by alcohol use. This may be a precursor to ongoing drinking problems and the precipitation of mental health problems.
- Child development can be adversely affected when women consume alcohol when pregnant or breast feeding. In particular drinking during pregnancy may lead to fetal alcohol syndrome a condition with ongoing physical, intellectual and behavioral dimensions.
This next table provides information about Australians episodic drinking (ie the number of drinks consumed during a single drinking session)
| Standard drinks per drinking episode | % Australians over 14 yrs. |
| Abstainers | 24 |
| Never exceed 4 std. drinks | 16 |
| 5-10 std. drinks less than monthly | 12 |
| 5-10 std. drinks at least monthly | 25 |
| 11+ std. drinks less than monthly – | 16 |
| 11+ std. drinks more than monthly – | 7 |
The guidelines also suggest that consumption of alcohol should not exceed 4 standard drinks during any drinking episode. 40% of Australians over 14 yrs are either abstainers or drinkers who limit their consumption to a maximum of four standard drinks on all occasions. 12% having occasional drinking episodes (binges) in which in which they drink more than 4 standard drinks. The remaining 48% have more frequent and/or heavier binges. The heavier the binge the greater the risk of one or more of the following adverse effects:
- unpleasant hangovers that may interfere with workplace attendance and productivity
- extreme intoxication requiring emergency medical care (particularly when combined with prescription or street drugs)
- accidental injury/death from falls, traffic accidents etc
- public drunkenness, disorderly behavior
- drink driving causing injury to the drinker, passengers and other road users.
- aggressive behavior causing injury to the drinker and/or others,
- unsafe sex/sexual assault perpetrated or experienced by the drinker
Despite the risks, binge drinking was traditionally a largely acceptable and at times celebrated aspect of male recreational behavior in Australia.
Women, however, were expected to show restraint in their drinking behavior. On the other hand, being drunk at work or drunk and disorderly in public places was frowned upon and those who repeatedly crossed this line faced sanctions and risked reputational damage.
Whilst there appears to be an increasing awareness of both the long and short term effects of alcohol misuse, the burden of alcohol related problems is still substantial. Recent data indicates that, annually, there are 1317 deaths in Australia that can be directly attributed to alcohol use. Alcohol has also been a contributory factor in the deaths of another 4504 Australians each year. Significantly, it is now been recognized that as many as 75% of people misuse alcohol also suffer from concurrent psychiatric co-morbidities such as anxiety, depression, bi-polar disorder, obsessive compulsive disorder and schizophrenia. Knowledge of this co-morbidity is crucial to the treatment of alcohol misuse and the related mental health issues. It’s also important to recognise the links between homelessness and alcohol misuse/dependence, where there is a complex system of reciprocal causalities. Alcohol misuse may lead to homelessness whilst homelessness may also precipitate or perpetuate alcohol misuse/dependence. Falls and other accidental injuries can often be linked to alcohol intoxication. Those of us who have had a fall outside the pub can relate to this! In addition to mental illness, there a long list of medical problems such as cardio-vascular conditions, kidney/liver/pancreas problems can be linked to alcohol consumption.
Like dependence on Nicotine, when someone becomes alcohol dependent it’s difficult to stop or reduce the level of drinking: due to physical, psychological and behavioral withdrawal symptoms. Sometimes symptoms are so severe and require hospitalization if abstinence is to be achieved. The Alcohol Use Disorders Identification Test (AUDIT) is a 10-item screening tool developed by the World Health Organization (WHO) to assess alcohol consumption, drinking behaviors, and alcohol-related problems.
Alcohol misuse is usually associated with a range of other legal and personal difficulties:
- Interpersonal problems including separation and alienation from family and friends.
- Financial problems Chronic inability to meet budget and meet financial commitments. Heavy alcohol use often leads to ongoing debt and other financial problems.
- Employment issues Intoxication and associated health and personal problems may have such an impact on heavy drinkers that they are unable to retain employment.
- Involvement in a range of delinquent behaviors such as public drunkenness and disorder, drink driving, physical assaults, shoplifting etc. This inevitably leads to police involvement, court appearances and possible incarceration.
Illegal drugs.
Recently published statistics indicate that around 57% of

Australians aged 14 years and over have never used street drugs or illegally obtained prescribed drugs. 26% of the population are ex-users and 17% are current users. Table 5 lists the most commonly used illegal drugs:
| Category of Drug | Examples | % Using |
| Cannabis | Marijuana (weed), Hashish (resin) | 11.6 |
| Ecstasy | 3.00 | |
| Meth/amphetamine | Crystal Meth (Ice) | 1.3 |
| Cocaine | 4.2 | |
| Hallucinogens | Ketamine, magic mushrooms | 1.6 |
| Inhalants | Glue, Petrol, Aerosols | 1.4 |
| Pain Medications | Codeine, Oxycontin Fentanyl | 2.7 |
| Tranquillizers | Valium, Nembutal, Zolpidem | 1.8 |
Unlike the other major recreational intoxicants, tobacco and alcohol, it’s somewhat difficult to gather reliable and consistent information about street drugs. For obvious reasons the activities of manufacturers, suppliers and retailers are shrouded in secrecy. Consequently accurate information about the chemical composition, strength, purity of street drugs is not available: nor is sales data . Proxy measures, such as illegal drug seizures, crime statistics, hospital emergency admissions etc can provide some information.
It is common for adolescents to start using illegal drugs: after all it is a fun activity! However, unregulated drug use is quite risky and can result in a variety of immediate unanticipated adverse outcomes such as accidental overdoses, hyperthermia, sexual and other forms of assault, STD’s, infections caused by unsterile injections etc. Fortunately most young people survive this experimentation and do not become drug dependent.

However, as with alcohol, the use of marihuana and other street drugs poses a risk to the still growing adolescent brain and can lead to an increased risk of subsequent mental illness. As the manufacture and supply of street drugs is completely unregulated, their use is inherently risky and therefore its impossible to provide advice about their use, apart from don’t.
Dependence on illegal drugs is in many ways quite similar to alcohol dependence and, of course, a significant number of drug users also misuse alcohol. For drug dependent users, recovery means coping with withdrawal symptoms in a somewhat way similar to that experienced by alcohol dependent people who are undergoing detoxification . Those dependent on illegal drugs, do have the additional problem of shopping for supplies in an illegal marketplaces. For some users, this can be very expensive and they resort to shoplifting, car theft, burglary and other forms of crime to pay their drug bills. Understandably, those affected by this drug related crime feel aggrieved and in some cases traumatized. This adds to the disapproval and stigma attached to all forms of illegal drug use.
An estimated 65% of prison entrants in Australia had used illicit drugs in the past year, compared to about 16% among the general population. The most common drugs used were methamphetamine, cannabis, pain killers and sleeping pills. Almost half of the people in prison reporting having injected drugs at some point in their life and two-thirds having injected drugs in the past year. Injecting drug use poses risks associated with the transmission of bloodborne viruses, both in and out of the prison system. With almost one in five people reporting the sharing of injecting equipment while in prison, there is a significant chance of hepatitis B and C transmission.
The deaths of 1865 Australians each year can be directly attributed to their use of illicit drugs. However it is probable that there are many other deaths, illnesses and injuries that are indirectly due to illicit drug use
wHAT SHOULD WE DO?
The use of intoxicating substances is a pleasurable activity which has occurred in most countries throughout the history of civilization. Like many pleasures it can present risks : occasionally these risks may be extreme.
In my opinion there is little to be gained and a lot to be lost in characterizing those who misuse alcohol and other drugs as self-indulgent, weak-willed, anti-social delinquents. This leads to a reliance on punitive measures to deal with the harms that some substance misusers can cause to themselves and those around them. My contention is that punitive measures should be regarded as a last resort, as there is very limited evidence of their effectiveness. Indeed, the long running “war on drugs” has proved to be a resounding failure because it fails to address the underlying economic, social and health problems which drive substance abuse and instead has relied on the “correction” of substance abuse through legal action and incarceration. Having stated this, I must acknowledge that there are no quick and easy alternatives. I would suggest that instead we we can progress by focusing on a number of broad principles that point to effective ways of reducing the harmful impact of substance misuse:
Most Australians successfully self regulate their use of alcohol and drugs by moderating their usage or abstaining, and I believe that it is important to acknowledge this.
- There is well established evidence of higher levels of smoking and alcohol and drug misuse in economically and socially disadvantaged communities. Reducing the impacts of this economic and social disadvantage is, therefore a basic pre-requisite to effective reduction of substance misuse. In our market driven, free enterprise economies, there will always be inequalities. However there are a number of obvious ways by means of which the impact of these inequalities can be significantly reduced. A prime example is workplace reforms that enshrine fair pay and conditions and enhance job security. Similarly the provision of affordable housing is a basic requisite for health and well-being.
- In the first instance substance abuse should be regarded as a health problem and interventions to limit health related harms should be regarded as a priority. For example methadone and other drug replacement programs needle exchange and safe injecting programs, pill testing at music festivals, decriminalization of marihuana, community based, homeless accommodation and sobering up facilities with case finding arrangements.
- Health practitioners, police officers and other front line workers need to have the capacity to recognize the many consumers who have concurrent mental health and substance abuse problems and endeavor to refer them to an appropriate range of treatment and support options.
- Currently many alcohol and drug awareness programs are school based. The effectiveness of these programs could be greatly increased by the use of a coordinated multi-level approach which encompassed the use of various mass media, information awareness and support for families and communities and school and other youth based interventions.
- The development of diversion programs should be escalated to reduce the drug and alcohol user population within correctional facilities. Similarly the number and scope of pre and post release programs for prisoners should be escalated to reduce alcohol and drug misuse following release.
Some suggested reading
- Global status report on alcohol and health 2018 : World Health Organization 2018
- Alcohol, tobacco & other drugs in Australia: Australian Institute of Health & Welfare 2021
- Alcohol risk and harm: Australian Institute of Health & Welfare 2021
- The Connection Between Substance Use Disorders and Mental Illness. https://www.drugabuse.gov/publications/research-reports/common-comorbidities-substance-use-disorders/part-1-connection-between-substance-use-disorders-mental-illness on 2021, October 28
- Under the Influence: A History of Alcohol in Australia: Fitzgerald R & Jordan TR
- Bob Hawke: Demons and Destiny: Bramston T 2022
- Social Determinants of Drug Use: National Drug and Alcohol Research Centre UNSW 2004
- National Drug Strategy 2017 – 2026: Australian Government Department of Health
- Understanding Alcohol Use Disorder – National Institute on Alcohol Abuse 2020
- Relapse – Alcohol and Drug Foundation https://adf.org.au/reducing-risk/relapse
- Drug and alcohol rehabilitation– Health Direct (Australian Government) https://www.healthdirect.gov.au/
